CME For the month of august 2013

WEST NILE FEVER
West
Nile Virus (WNV) can cause neurological disease and death in people. WNV is
commonly found in Africa, Europe, the Middle East, North America and West Asia.
WNV is maintained in nature in a cycle involving transmission between birds and
mosquitoes. Humans, horses and other mammals can be infected.WNV is a member of
the flavivirus genus and belongs to the Japanese
encephalitis antigenic complex of the family Flaviviridae.Virus was first isolated in a woman in the West Nile district of
Uganda in 1937. It was identified in birds (crows and columbiformes) in Nile
delta region in 1953.
·
West Nile virus
can cause a fatal neurological disease in humans.
·
However,
approximately 80% of people who are infected will not show any symptoms.
·
West Nile virus
is mainly transmitted to people through the bites of infected culux mosquitoes.The
virus can cause severe disease and death in horses. Since WNV
outbreaks in animals precede human cases, the establishment of an active animal
health surveillance system to detect new cases in birds and horses is essential
·
Vaccines are
available for use in horses but not yet available for people.
·
Birds are the
natural hosts of West Nile virus.
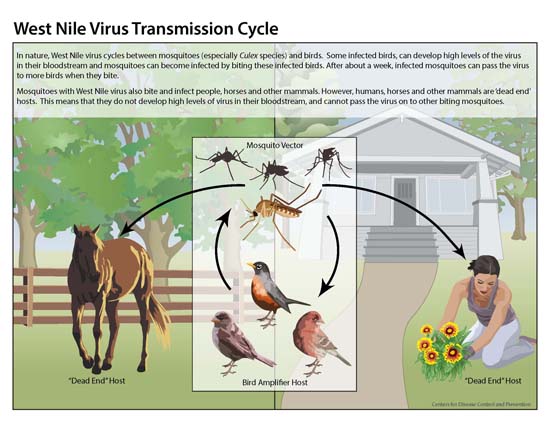
Transmission
Human infection is most often the result of bites from
infected mosquitoes. Mosquitoes become infected when they feed on infected
birds, which circulate the virus in their blood for a few days. The virus
eventually gets into the mosquito's salivary glands. During later blood meals
(when mosquitoes bite), the virus may be injected into humans and animals,
where it can multiply and possibly cause illness.
The virus may also be transmitted through contact with
other infected animals, their blood, or other tissues.
A very small proportion of human infections have occurred
through organ transplant, blood transfusions and breast milk. There is one
reported case of transplacental (mother-to-child) WNV transmission.
To date, no human-to-human transmission of WNV through
casual contact has been documented, and no transmission of WNV to health care
workers has been reported when standard infection control precautions have been
put in place.
Transmission of WNV to laboratory workers has been
reported. . Samples taken
from people and animals with suspected WNV infection should be handled by
trained staff working in suitably equipped laboratories.
SIGNS AND
SYMPTOMS
Infection with WNV is either asymptomatic in around 80%
of infected people, or can lead to West Nile fever or severe West Nile disease.
About 20% of people who become infected with WNV will develop West Nile fever.
Symptoms include fever, headache, tiredness, and body aches, nausea, vomiting,
occasionally with a skin rash (on the trunk of the body) and swollen lymph
glands.
The symptoms of severe disease (also called neuroinvasive
disease, such as West Nile encephalitis or meningitis or West Nile
poliomyelitis) include headache, high fever, neck stiffness, stupor,
disorientation, coma, tremors, convulsions, muscle weakness, and paralysis. It
is estimated that approximately 1 in 150 persons infected with the West Nile
virus will develop a more severe form of disease. Serious illness can occur in
people of any age, however people over the age of 50 and some immunocompromised
persons (for example, transplant patients) are at the highest risk for getting
severely ill when infected with WNV.
The incubation period is usually 3 to 14 days.
DIAGNOSIS
West Nile virus can be diagnosed by a number of different
tests:
·
IgG antibody
sero-conversion (or significant increase in antibody titers) in two serial
specimen collected at a one week interval by enzyme-linked immunosorbent assay
(ELISA);
·
IgM antibody
capture enzyme-linked immunosorbent assay (ELISA);
·
neutralisation
assays;
·
viral detection
by reverse transcription polymerase chain reaction (RT-PCR) assay, and
·
virus isolation
by cell culture.
IgM can be detected in nearly all cerebrospinal fluid
(CSF) and serum specimens received from WNV infected patients at the time of
their clinical presentation. Serum IgM antibody may persist for more than a
year.
TREATMENT AND
VACCINE
Treatment is supportive for patients with neuro-invasive
West Nile virus, often involving hospitalization, intravenous fluids,
respiratory support, and prevention of secondary infections. No vaccine is
available for humans.
VECTOR AND
ANIMAL HOSTS
WN virus is maintained in nature in a
mosquito-bird-mosquito transmission cycle. Mosquitoes of the genus Culex are generally
considered the principal vectors of WNV, in particular Cx. Pipiens. WNV is maintained in mosquito populations through
vertical transmission (adults to eggs).
Birds are the reservoir hosts of WNV. In Europe, Africa,
Middle East and Asia, mortality in birds associated with WNV infection is rare.
Members of the crow family (Corvidae) are particularly susceptible, but
virus has been detected in dead and dying birds of more than 250 species. Birds
can be infected by a variety of routes other than mosquito bites, and different
species may have different potential for maintaining the transmission cycle.
Horses, just like humans, are “dead-end” hosts, meaning
that while they become infected, they do not spread the infection. Symptomatic
infections in horses are also rare and generally mild, but can cause neurologic
disease, including fatal encephalomyelitis.
Prevention- Effective
prevention of human WNV infections depends on the development of comprehensive,
integrated mosquito surveillance and control programmes in areas where the
virus occurs. Studies should identify local mosquito species that play a role
in WNV transmission, including those that might serve as a “bridge” from birds
to human beings. Emphasis should be on integrated control measures including
source reduction (with community participation), water management, chemicals,
and biological control methods.
Reducing the
risk of infection in people
In the absence of a vaccine, the only way to reduce
infection in people is by raising awareness to reduce exposure to the virus.
·
Reducing the
risk of mosquito transmission. Efforts to prevent transmission should first
focus on personal and community protection against mosquito bites
·
Reducing the
risk of animal-to-human transmission. Gloves and other protective clothing
should be worn while handling sick animals or their tissues, and during
slaughtering and culling procedures.
Reducing the risk of transmission through blood
transfusion and organ transplant. Blood and organ donation restrictions and
laboratory testing should be considered at the time of the outbreak in the
affected areas after assessing the local/regional epidemiological situation.
WEST NILE VIRUS IS MOST COMMONLY TRANSMITTED TO HUMANS BY
MOSQUITOES.ADDITIONAL ROUTES OF HUMAN INFECTION HAVE ALSO BEEN DOCUMENTED.BUT
THESE METHODS OF TRANSMISSION REPRESENT A VERY SMALL PROPORTION OF CASES:
·
BLOOD TRANSFUSIONS
·
ORGAN TRANSPLANTS
·
EXPOSURE IN A LABORATORY SETTING
·
FROM MOTHER TO BABY DURING PREGNANCY,
DELIVERY, OR BREASTFEEDING
WEST NILE VIRUS IS NOT TRANSMITTED:
·
FROM PERSON-TO-PERSON OR FROM
ANIMAL-TO-PERSON THROUGH CASUAL CONTACT. NORMAL VETERINARY INFECTION CONTROL
PRECAUTIONS SHOULD BE FOLLOWED WHEN CARING FOR A HORSE SUSPECTED TO HAVE THIS
OR ANY VIRAL INFECTION.
·
FROM HANDLING LIVE OR DEAD INFECTED
BIRDS. YOU SHOULD AVOID BARE-HANDED CONTACT WHEN HANDLING ANY DEAD ANIMAL. IF
YOU ARE DISPOSING OF A DEAD BIRD, USE GLOVES OR DOUBLE PLASTIC BAGS TO PLACE
THE CARCASS IN A GARBAGE CAN.
·
THROUGH CONSUMING INFECTED BIRDS OR
ANIMALS. IN KEEPING WITH OVERALL PUBLIC HEALTH PRACTICE, AND DUE TO THE RISK OF
KNOWN FOOD-BORNE PATHOGENS, ALWAYS FOLLOW PROCEDURES FOR FULLY COOKING MEAT
FROM EITHER BIRDS OR MAMMALS.